Recording
Records should be made as soon as possible after the incident is resolved. This includes a description of what happened, the date and who was affected. Recording what action was taken helps to ensure harm to the patient was avoided or reduced.
Reporting
Reporting incidents improves understanding of what is going wrong in the company, organisation or healthcare nationally. Every report submitted to the NRLS is valuable. Analysis of these reports has greatly aided understanding of the biggest medication risks, improving our ability to respond.
Significant Event Audit (SEA)
An SEA involves an analysis of the incident and its benefits from a team approach. The opportunity to use the skills of the wider team, particularly technicians, should be considered. The analysis of the event is broken down into four stages:
1. Describe what happened: this is where the results of the factfinding or investigation are presented and the error defined
2. Why did it happen? List the possible contributory factors
3. What have we learned? E.g. €This {insert contributory factor} needs to be addressed to reduce the chance of {insert error} happening again€
4. What will we change? What might be changed should be discussed.
Lessons and actions
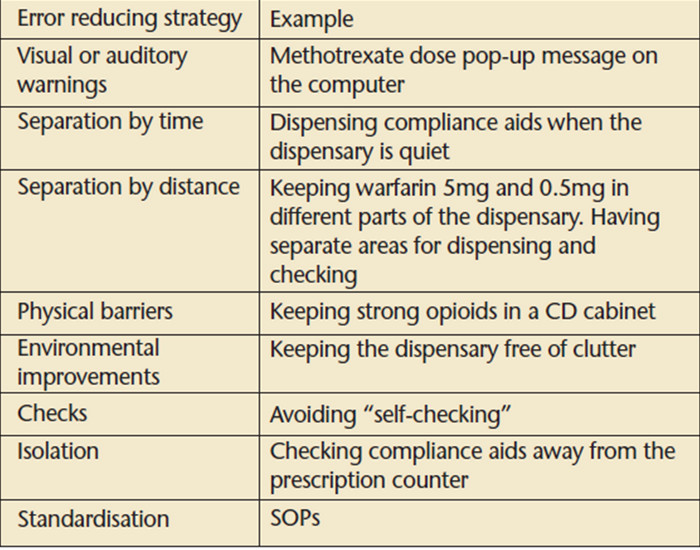
Reducing errors is best achieved by addressing the factors that are influential in causing errors. However, deciding what can be done can prove challenging. Care should be taken not to change things for the worse. Strategies that could be considered to reduce the risk of error are described in table 2. There are still many lessons to be learnt from the alerts, notices and rapid response reports published by the National Patient Safety Agency.
Table 2: strategies to prevent error